Dietary fish oil can positively impact sperm parameters and improve male fertility
Posted By Braverman IVF & Reproductive Immunology || 08-Jan-2018
Male fertility is defined as the ability of a man to impregnate a healthy, fertile woman of reproductive age.
Twelve percent of women aged 15 to 44 years in the United States have difficulty getting pregnant or carrying a pregnancy to term as stated by The Center for Diseases Control and Prevention (CDC).
In about 35% of these infertile couples (unable to conceive a child despite unprotected sexual intercourse for at least a year), a male factor is identified along with a female factor while in 8% of couples with infertility, a male factor is the only identifiable cause. Diagnosing a male as fertile or infertile is quite difficult, as this status can vary over short periods of time and even with different partners.
Estimating male fertility potential relies mostly on a sperm analysis that evaluates:
- Volume of semen ejaculate
- Sperm concentration
- Motility of spermatozoa
- Percentage of normal shaped-spermatozoa
- Semen inflammation status
At Braverman Reproductive Immunology, in addition to sperm analysis, we are now starting to look at the immune system and inflammation as it relates to male factor infertility.
Male infertility: Causes
Male infertility is due to low sperm production, abnormal sperm function or blockages that prevent the delivery of sperm. The reasons for poor semen quality and low sperm quantity are not yet fully established but some associations have been shown with:
- an inherited disorder such as Klinefelter syndrome (XXY) or a microdeletion of the Y chromosome
- hormonal imbalance
- lifestyle choices such as smoking, illicit drugs or alcohol consumption
- underlying medical conditions such as diabetes or obesity
A recent meta-analyze (1) that includes 185 studies conducted between 1973 and 2011, and involving almost 43,000 fertile men showed a dramatic decrease in the concentration of sperm of men from western countries dropping to -52% over a 40 years period.
Potential causes are multiple and could be attributed to obesity, stress, chemical and electromagnetic exposures leading to endocrine disruption and detrimental reproductive effects.
Sperm DNA damage: a key player in male infertility
If the use of biotechnologies of reproduction such as In Vitro Fertilization (IVF) or Intracytoplasmic sperm injection (ICSI) could help achieve a pregnancy despite low sperm count, the higher rate of sperm abnormal morphology has been widely described and is a main concern. Indeed, many studies reported the higher incidence of abnormal sperm infertile couples.
The Study for Future Families (SFF) measured semen parameters in 763 partners of pregnant women in several states of the United States (CA, MN, MO, NY and IA) and showed a decreased in sperm motility and higher rate of abnormal sperm morphology in rural areas (3). Another recent study of young men from the general Danish population showed that the median percent of morphologically normal spermatozoa is ∼7% only (4)
The presence of sperm with abnormal morphology indicates that spermatozoa did not complete the entire process of maturation (from spermatid to mature and motile spermatozoa) and could reveal sperm DNA damage based on studies showing a negative relationship between sperm chromatin (DNA) quality and sperm parameters including morphology and motility (5, 6).
Human sperm DNA damage affects male fertility as seen by many studies showing the increased rate of spermatozoa with abnormal chromatin in infertile patients when they are compared with fertile men (7-8).
Sperm DNA damage can be induced by multiple factors as seen in Figure1.
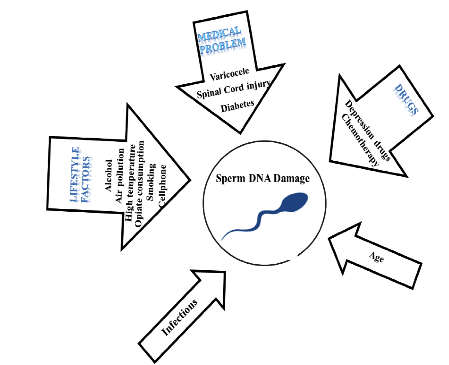
Figure 1. Etiological factors associated with increased human sperm damage
from Pourmasuhi, 2014 (9).
Among them, lifestyle factors and particularly diet could have severe detrimental effects on sperm DNA integrity thus impacting male fertility.
A systematic review investigated the effect of paternal obesity on reproductive potential on over 1154 000 men showed that obese men were more likely to experience infertility (9-10). This could be imputed to:
- A higher percentage of sperm with DNA fragmentation
- An increased percentage of sperm with disrupted mitochondrial function (low mitochondrial membrane potential)
- An increased percentage of spermatozoa with abnormal morphology.
It is important to note that the conventional semen parameters (volume, concentration, motility) were not found to be different between lean and obese males, highlighting the need of a sperm DNA fragmentation test to estimate semen quality and detect patient at higher risk for infertility (11).
Obesity causes an increase in systemic inflammation that results in an increased production of reactive oxygen species (oxidative stress) (12) and this, in turn is associated with damage to cellular biomolecules such as DNA, in addition to deregulating the acrosome reaction (activation of the spermatozoa in contact to the oocyte) and disrupting the sperm–oocyte recognition and fusion (13) which lower the odd for the fertilization to occur to form an embryo.
Omega 3: a natural solution to improve your sperm’s parameters
Many cases of male infertility are diagnosed as idiopathic and remained untreated. As seen in the previous section, the significant decrease in semen parameters over the years could be, at least partially, attributed to a poor diet with low intake of antioxidant nutrients and an alimentation rich in sugar and saturated fatty acid (14-15). Fatty acids (FAs) are classified based on the number of carbons that determines their lengths and the number of unsaturation (double bonds) that confer them specific properties. Fatty acid brought to your system in the form of triglyceride (by your diet) are a source of energy for your body.
There are three types of natural FAs:
- Saturated
- Monounsaturated
- Polyunsaturated
Polyunsaturated fatty acids (PUFAs) are essential FAs, because they cannot be synthesized by the human body. Both omega 3 and omega 6 polyunsaturated fatty acids are essential components of phospholipids present in all tissues including spermatozoa cell membranes (16) whose potential for a successful fertilization relies on its membrane lipid composition (17). The precursors of the omega 3 (alpha -linoleic acid: ALA) will give rise to two ω3 fatty acids: EPA and DHA (collectively referred as the omega 3), that play a major role in reducing inflammation and oxidative stress.
The linoleic acid (LA, precursor of the ω6 pathway) will give rise to the arachidonic acid (AA) that is pro-inflammatory. Although some omega 6 fatty acid (dihomo-γ-linolenic acid) could have anti-inflammatory properties, the ω6 pathway is considered as pro-inflammatory whereas the ω3 pathway is anti-inflammatory (18-19).
Living in a westernized country, we have a diet that is very rich in omega 6 (processed food, fast-food, lots of meat, low amount of vegetables), therefore our ratio between omega 6 and omega 3 (ω6/ω3) is very high, reaching value of 20 or more (20). This ratio, reflecting our propensity to stimulate anti- (ω3) or pro-inflammatory (ω6) pathways could be modulated by changes in your diet. Indeed, by reducing your ω6 intake (more vegetables, less meat) and increasing your omega 3 intakes by eating more fish and sea food, this could help establish a more balanced 𝜔6𝜔3 ratio on the long term. An easier and faster way to optimize your 𝜔6𝜔3 ratio is to supplement your diet with omega 3 fish oil rich in EPA and DHA.
Fatty acid profile in relation to sperm parameters While the intake of omega‑3 polyunsaturated fatty acids has been shown to be associated with a better testicular function as indicated by higher testicular volume (21), other studies analyzing the fatty acid (FA) composition of spermatozoa of normozoospermic, asthenozoospermic (reduced sperm motility), oligozoospermic (low sperm concentration) and oligoasthenozoospermic men (low sperm concentration and reduced motility) showed an increased omega-6/omega-3 ratio in men’s spermatozoa with impaired semen quality (22). In addition, another similar study showed a strong association between DHA and sperm motility, sperm concentration and normal sperm morphology (23). Interestingly, fatty acid levels in the blood correlates with fatty acid levels in the semen.
Indeed, in studies investigating the PUFA composition of the blood plasma and spermatozoa of fertile men as compared to infertile men (24-25), results showed:
- higher blood and spermatozoa levels of omega-3 PUFAs in fertile men compared with the infertile counterparts.
- serum 𝜔6𝜔3 ratio was significantly higher in infertile men.
- Potential for inflammation as defined by AA/EPA ratio was higher in infertile men.
Another study confirmed these findings in N=99 men where higher omega 3 PUFA intake correlates with better sperm morphology (26) but also better sperm motility and viability after freezing/thawing (27).
How much omega 3 do men need?
There is an abundance of literature about fish oil/omega 3 supplementation studies improving semen parameters in animal (28-31) but studies are limited in men. In a study on healthy, young men (32) when a source of omega 3 is administrated (75 g of walnuts per day for 12 weeks), leading to increased DHA levels, results showed an improvement in:
- Sperm vitality
- Sperm motility
- Sperm morphology
In another study (33), a supplementation with DHA (400 or 800mg/day for 3 months) in men with asthenozoospermia (decreased motility) showed in the serum:
- a significant decrease in the omega 6 pathway (−31%) in the 800mg group only
- a significant decrease in the 𝜔6𝜔3 ratio in the 400 and 800 mg supplemented groups (34.9 and 33.3%, respectively).
- an increased in DHA levels (37 and 40% in the 400 and 800 mg DHA groups, respectively)
- an increased in total n-3 fatty acids (33 and 30% in the 400 and 800 mg DHA groups, respectively).
Nevertheless, little effect has been noted at the sperm level (slight decrease in total omega 6 but no impact on sperm motility or concentration). These limited effects are in opposition with other studies. Indeed, in a large-scale study (34), 266 infertile men with idiopathic oligoasthenozoospermia (OAT) were randomly assigned to fish oil treatment that contained EPA and DHA, at doses of 1.84 g per day or placebo that contained corn oil for a relatively long duration of 32 weeks.
Results showed that in the treatment group:
- EPA and DHA levels in blood and seminal plasma showed a statistically significant correlation with those in the spermatozoa.
- a significant improvement of sperm cell total count and sperm cell concentration in the fish oil group.
Similarly, in a study (35) including oligozoospermic men (low sperm concentration), dietary supplementation (1g DHA/day in addition to oral anti-oxidant) showed:
- increase in sperm concentrations (7.4 vs. 12.5 million/ mL)
- increase of the acrosome reaction (55 vs. 71%): step allowing the penetration of the spermatozoa to fertilize the egg
- significant reduction of oxidative stress with decreased in ROS levels (775 vs. 150 (1000 counts/10 second)
Interestingly, a DHA dietary supplementation for 10 weeks at 1.5g/day (36) is able by itself to induce an increase in total antioxidant capacity with a significant reduction in the percentage of spermatozoa with DNA damage.
Altogether, these studies showed the beneficial impact of omega 3 in sperm parameters. Omega 3 levels in sperm correlate with serum levels and can be modulated by dietary omega 3 (EPA+DHA) supplementation to improve male fertility.
At Braverman Reproductive Immunology, we will shortly begin screening all male patients for fatty acid levels when prior low embryo quality was observed, in addition to abnormal sperm analysis. Further, we start looking at the immune system and inflammation as it relates to male factor infertility.
Based on our previous work in female patients, we have determined three parameters:
- ω6/ω3 ratio
- Potential for inflammation reflecting the direct competition between EPA and arachidonic acid in triggering pro- versus anti-inflammatory pathway.
- Omega 3 Index: this index reflecting the long-term intake of EPA+DHA has been largely used in the cardiovascular medical field to determine patients who are in a protective zone versus those at risk for cardiac arrest
Based on these parameters, patients are categorized into one of three categories:
- Low risk
- Intermediate risk
- High risk
Specific dose of EPA+DHA are recommended to restore optimum parameters before a subsequent attempt to conceive.
References
1. Levine H, Jørgensen N, Martino-Andrade A, Mendiola J, Weksler-Derri D, Mindlis I, Pinotti R, Swan SH. Temporal trends in sperm count: a systematic review and meta-regression analysis. Hum Reprod Update. 2017 Nov 1;23(6):646-659.
2. Skakkebaek NE, Rajpert-De Meyts E, Buck Louis GM, Toppari J, Andersson AM, Eisenberg ML, Jensen TK, Jørgensen N, Swan SH, Sapra KJ, Ziebe S, Priskorn L, Juul A. Male Reproductive Disorders and Fertility Trends: Influences of Environment and Genetic Susceptibility. Physiol Rev. 2016 Jan;96(1):55-97.
3. Redmon JB, Thomas W, Ma W, Drobnis EZ, Sparks A, Wang C, Brazil C, Overstreet JW, Liu F, Swan SH. Semen parameters in fertile US men: the Study for Future Families. Andrology 1: 806–814, 2013.
4. Jørgensen N, Joensen UN, Jensen TK, Blomberg Jensen M, Almstrup K, Olesen IA, Juul A, Andersson AM, Carlsen E, Petersen JH, Toppari J, Skakkebæk NE. Human semen quality in the new millennium: a prospective cross-sectional population-based study of 4867 men. BMJ Open 2: e000990, 2012.
5. Larson-Cook KL, Brannian JD, Hansen KA, Kasperson KM, Aamold ET, Evenson DP. Relationship between the outcomes of assisted reproductive techniques and sperm DNA fragmentation as measured by the sperm chromatin structure assay. Fertil Steril 2003; 80: 895-902.
6. Giwercman A, Richthoff J, Hjøllund H, Bonde JP, Jepson K, Frohm B, et al. Correlation between sperm motility and sperm chromatin structure assay parameters. Fertil Steril 2003; 80: 1404-1412.
7. Machev N, Gosset P, Viville S. Chromosome abnormalities in sperm from infertile men with normal somatic karyotypes: teratozoospermia. Cytogen Genome Res 2005; 111: 352-357.
8. Zini A, Libman J. Sperm DNA damage: clinical significance in the era of assisted reproduction. Canadian Med Assoc J 2006; 175: 495-500.
9. Pourmasumi S, Sabeti P, Rahiminia T, Mangoli E, Tabibnejad N, Talebi AR. The etiologies of DNA abnormalities in male infertility: An assessment and review. Int J Reprod Biomed (Yazd). 2017 Jun;15(6):331-344. Review.
10. Campbell JM, Lane M, Owens JA, Bakos HW. Paternal obesity negatively affects male fertility and assisted reproduction outcomes: a systematic review and meta-analysis. Reprod Biomed Online. 2015 Nov;31(5):593-604.
11. Agarwal A, Said TM 2003a Role of sperm chromatin abnormalities and DNA damage in male infertility. Human Reproduction Update 9, 331–345.
12. Kahn BE, Brannigan RE. Obesity and male infertility. Curr Opin Urol. 2017Sep;27(5):441-445.
13. Agarwal A, Saleh RA, Bedaiwy MA 2003. Role of reactive oxygen species in the pathophysiology of human reproduction. Fertility and Sterility 79, 829–843.
14. Mendiola J, Torres-Cantero AM, Vioque J, Moreno-Grau JM, Ten J et al. A low intake of antioxidant nutrients is associated with poor semen quality in patients attending fertility clinics. Fertil Steril 2010; 93: 1128–33.
15. Vujkovic M, de Vries JH, Dohle GR, Bonsel GJ, Lindemans J. Associations between dietary patterns and semen quality in men undergoing IVF/ ICSI treatment. Hum Reprod (Oxford, England) 2009; 24: 1304–12.
16. Mazza M, PomponiM, Janiri L, Bria P,Mazza S. Omega- 3 fatty acids and antioxidants in neurological and psychiatric diseases: an overview. Prog Neuropsychopharmacol Biol Psychiatry 2007; 31: 12–26.
17. Lenzi A, Gandini L, Maresca V, Rago R, Sgro P. Fatty acid composition of spermatozoa and immature germ cells. Mol Hum Reprod 2000; 6: 226–31.
18. Anderson BM, D.W.Ma, Areall. n-3 polyunsaturated fatty acids created equal? Lipids HealthDis.8(2009)1.
19. Calder PC. Omega-3polyunsaturatedfattyacidsandinflammatory processes: nutrition orpharmacology? Br.J.Clin. Pharmacol.75 (2013)645–662.
20. Weaver KL, Ivester P, Seeds M, Case LD, Arm JP et al. Effect of dietary fatty acids on inflammatory gene expression in healthy humans. J Biol Chem 2009; 284: 15400–7.
21. MInguez-Alarcón L, Chavarro JE, Mendiola J, Roca M, Tanrikut C, Vioque J, Jørgensen N, Torres-Cantero AM. Fatty acid intake in relation to reproductive hormones and testicular volume among young healthy men. Asian J Androl. 2017 Mar-Apr;19(2):184-190.
22. Aksoy Y, Aksoy H, Altinkaynak K, Aydin HR, Ozkan A. Sperm fatty acid composition in subfertile men. Prostaglandins Leukot Essent Fatty Acids 2006; 75: 75–9.
23. Conquer JA, Martin JB, Tummon I, Watson L, Tekpetey F. Fatty acid analysis of blood serum, seminal plasma, and spermatozoa of normozoospermic vs. asthenozoospermic males. Lipids 1999; 34: 793–9.
24. Safarinejad MR, Hosseini SY, Dadkhah F, Asgari MA. Relationship of omega-3 and omega-6 fatty acids with semen characteristics, and anti-oxidant status of seminal plasma: a comparison between fertile and infertile men. Clin Nutr 2010; 29: 100–5.
25. Safarinejad MR, Hosseini SY, Dadkhah F, Asgari MA. Relationship of omega-3 and omega-6 fatty acids with semen characteristics, and anti-oxidant status of seminal plasma: a comparison between fertile and infertile men. Clin Nutr 2010; 29: 100–5.
26. Attaman JA, Toth TL, Furtado J, Campos H, Hauser R. Dietary fat and semen quality among men attending a fertility clinic. Hum Reprod 2012; 27: 1466–74.
27. Martınez-Soto JC, Landeras J & Gadea J. (2013) Spermatozoa and seminal plasma fatty acids as predictors of cryopreservation success. Andrology 1, 365–375.
28. Alizadeh A, Esmaeili V, Shahverdi A, Rashidi L. Dietary Fish Oil Can Change Sperm Parameters and Fatty Acid Profiles of Ram Sperm during Oil Consumption Period and after Removal of Oil Source. Cell J. 2014 Fall;16(3):289-98.
29. Gholami H, Chamani M, Towhidi A, Fazeli MH. Effect of feeding a docosahexaenoic acid-enriched nutriceutical on the quality of fresh and frozen-thawed semen in Holstein bulls. Theriogenology. 2010 Dec;74(9):1548-58.
30. Gholami H, Chamani M, Towhidi A, Fazeli MH. Improvement of Semen Quality in Holstein Bulls during Heat Stress by Dietary Supplementation of Omega-3 Fatty Acids. Int J Fertil Steril. 2011 Jan;4(4):160-7.
31. Lin Y, Cheng X, Mao J, Wu D, Ren B, Xu SY, Fang ZF, Che LQ, Wu CM, Li J. Effects of different dietary n-6/n-3 polyunsaturated fatty acid ratios on boar reproduction. Lipids Health Dis. 2016 Feb 16;15: 31
32. Robbins WA, Xun L, FitzGerald LZ, Esguerra S, Henning SM & Carpenter CL. (2012) Walnuts improve semen quality in men consuming a Western-style diet: randomized control dietary intervention trial. Bio Reprod 87, 101–108.
33. Conquer JA, Martin JB, Tummon I, Watson L, Tekpetey F. Effect of DHA supplementation on DHA status and sperm motility in asthenozoospermic males. Lipids. 2000 Feb;35(2):149-54.
34. Safarinejad MR. (2011) Effect of omega-3 polyunsaturated fatty acid supplementation on semen profile and enzymatic anti-oxidant capacity of seminal plasma in infertile men with idiopathic oligoasthenoteratospermia: a double-blind, placebo-controlled, randomised study. Andrologia 43, 38–47.
35. Comhaire FH, Christophe AB, Zalata AA, Dhooge WS, Mahmoud AM, Depuydt CE. The effects of combined conventional treatment, oral antioxidants and essential fatty acids on sperm biology in subfertile men. Prostaglandins Leukot Essent Fatty Acids. 2000 Sep;63(3):159-65.
36. Martínez-Soto JC, Domingo JC, Cordobilla B, Nicolás M, Fernández L, Albero P, Gadea J, Landeras J. Dietary supplementation with docosahexaenoic acid (DHA) improves seminal antioxidant status and decreases sperm DNA fragmentation. Syst Biol Reprod Med. 2016 Dec;62(6):387-395