- Control of inflammation: a key parameter to establish and maintain a healthy pregnancy
Pregnancy is one of the most complex process requiring a fine-tune communication
between a receptive endometrium (uterus) and a developing and competent embryo.
This cross-talk is highly dependent on uterine microenvironment whose
dysregulation through untimely activation of inflammatory processes can
have devastating effects on pregnancy outcomes leading to miscarriages
or obstetrical complications including but not limited to pre-eclampsia,
preterm birth or even still birth.
A healthy pregnancy switches the maternal immune system toward a more tolerant,
low inflammatory state.
Many autoimmune diseases or other conditions such as PCOS or endometriosis
may lead to systemic inflammation and oxidative stress negatively impacting
oocyte/embryo quality and may be involved in infertility and recurrent
pregnancy loss (RPL). For more information,
read our blog on the topic.
It is crucial to minimize these uncontrolled inflammatory changes to allow
the establishment and the maintenance of a pregnancy.
- Omega 3: Fatty acid playing a key role in preventing inflammation
Fatty acids are classified based on the number of carbons that determines
their lengths and the number of unsaturation (double bonds) that confer
them specific properties. Fatty acid brought to your system in the form
of triglyceride (by your diet) are a source of energy for your body.
Thus,
the quality of the maternal diet
is directly impacting
maternal health,
pregnancy and fetal outcomes, as well as the risk of pregnancy complications.
In the below section, we will explain you how a category of fatty acid, the
Omega 3 (ω3) could have multiple beneficial effects on minimizing your inflammation
and improving your chance for a healthy pregnancy.
- Omega 6 and Omega 3: dichotomic pathways
Both omega 3 and omega 6 fatty acids are essential components of phospholipids
present in all tissues. They both synthesize lipids, support normal cell
function as well as fetal development (1).
The precursors of the omega 3 (alpha -linoleic acid: ALA) and omega 6 (linoleic
acid: LA) pathway are both essential fatty acids (your body can not synthesize
them) and must be obtain through your diet (2).
As seen in the simplified
Figure 1 below, ALA will give rise to two ω3 fatty acids: EPA and DHA (collectively
referred as
the omega 3), that
play a major role in reducing inflammation and oxidative stress.
LA (ω6 pathway) will give rise to the arachidonic acid (AA) that
is pro-inflammatory.
Although some omega 6 fatty acid (dihomo-γ-linolenic acid) could
have anti-inflammatory properties, the ω6 pathway is considered
as pro-inflammatory whereas the ω3 pathway is anti-inflammatory (3-4).
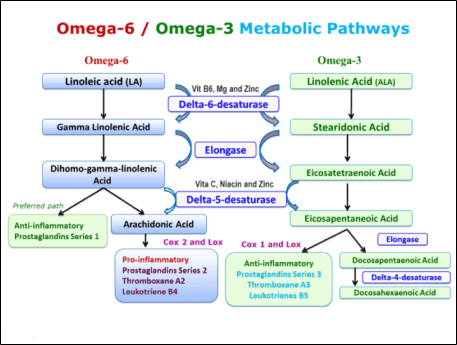
Figure 1: Omega 6 and omega 3 metabolic pathways.
The ω3 anti-inflammatory effects are multiple:
- It inhibits AA-derived eicosanoids by EPA incorporation to the membrane
phospholipid at the expense of AA (5).
- It inhibits the Toll Like Receptor/NFKB pathway and the enzyme COX2 (enzyme
responsible of the production of pro-inflammatory molecules) resulting
in the inhibition of pro-inflammatory cytokine production (6-7).
- It suppresses T lymphocyte activation (8).
- It induces the production of resolvin (derived from EPA and DHA), maresin
and protectin (derived from DHA only) which are potent anti-inflammatory
factors (9) and have been shown to play key roles in preventing several
pregnancy complications associated with excessive systemic and placental
inflammation (10).
The ω3 anti-oxidative properties (11-12) are triggered through:
- the inhibition of reactive oxygen species (ROS)
- reduction of peroxide production
- reduction of the enzyme activity NOS (involved in reactive species production).
-
Manipulating your fatty acid content through omega 3 supplement could restore
a more balanced ω6/ω3
ratio, help minimize
inflammation and be beneficial to pregnancy
- How can I improve my ω6/ω3?
Living in a westernized country, we have a diet that is very rich in omega
6 (processed food, fast-food, lots of meat, low amount of vegetables),
therefore our ratio between omega 6 and omega 3 (ω6/ω3) is
very high, reaching value of 20 or more.
This ratio, reflecting our propensity to stimulate anti- (ω3) or
pro-inflammatory (ω6) pathways could be modulated by changes in
your diet. Indeed, by reducing your ω6 intake (more vegetables,
less meat) and increasing your omega 3 intakes by eating more fish and
sea food, this could help established a more balanced ω6/ω3
ratio on the long term.
However, the efficiency of this process is generally very low. Indeed,
up to 35% of ALA (precursor substrate of the ω3 pathway) is catabolized into CO2 for energy and won’t be able to induce EPA/DHA formation. Further,
a diet richer in ALA will have higher rate of ALA oxidation (13).
In women, only 21% of ALA is converted to EPA and less than 9% gives rise
to DHA (14). Moreover, there is a big variability in subject capacity
to convert ALA to EPA/DHA even when the subjects have similar diet (15).
Therefore, the best option for a rapid and sustained change in ω6/ω3
ratio may be to directly supplement patient with EPA and DHA to short
cut their moderately effective synthesis from ALA.
- ω3 beneficial effects during pregnancy?
ω3 have been used for years to treat patients affected by cardiovascular
diseases and reduce their hyperlipidemia and has been proved to be totally safe.
When ω6/ω3 ratio goes from 10 to 4 in patient with cardiovascular
disorders, there is a reduction of 70% in mortality (16).
In fertility, an increased ω3 intake prior to conception was shown
to positively impact embryo morphology in a study on women undergoing
IVF cycle (17).
ω3 appear to promote vascular development in the endometrium as
seen by in vitro study (18). Many other studies showed that a higher ω3 intake:
- can reduce the risk of miscarriage (19).
- Increase uterine blood flow (20).
- Increase the length of pregnancy and reduce preterm birth (21).
- Reduce placental inflammation when taking during the first trimester and
through the pregnancy (22).
The figure below can summarize how ω3 can help reduce maternal inflammation/
oxidative stress (23). They directly act on placenta to increase anti-oxidant
production that will counteract the effects of reactive oxygen species
(ROS). Resolvins and protectins (products of DHA and EPA metabolism) can
reduce placental PGE2 (the prostaglandin associated with partition) and
reduce placental inflammation. Altogether, these effects can reduce the
risk of pregnancy losses or complications.
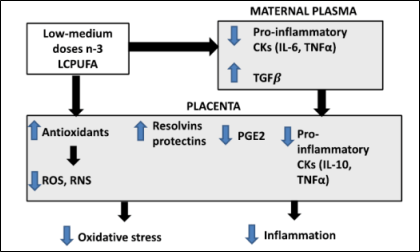
Figure 2: Summary of ω3 pleiotropic effects on maternal/placental inflammation
- Focus on our Intralipid study: what did we learn from our data?
- No significant effect of Intralipid in our patient population
Intralipid is a lipid emulsion (an emulsion containing ω3 and ω6
fatty acid among other fatty acid) used for over 50 years as an intravenous
nutrition method.
It is one of the
most used drug in fertility treatment whose use has showed a total safety
during pregnancy.
We tried to find any immunological evidences that could explain how Intralipid
infusion modulate maternal immune response thus allowing the establishment
and maintenance of pregnancy.
In our set of patients, Intralipid did not show any dramatic effects on
immune factors (no further reduction of NKa levels in pregnant patients
on Intralipid as compared to patients not using it). Further, Intralipid
was not shown to improve pregnancy rate (as compared to other therapies).
- Lower ω6/ω3 ratio at baseline linked pregnancy to success
We decided to focus on determining if Intralipid similarly modulate the
fatty acid content among patients. Strikingly, we found that patients
could respond in totally opposite way to Intralipid infusion (at the same
frequency and dosage).
Some patients will have significantly increased linoleic acid levels (LA,
ω6) while others will have a significant decrease in linoleic acid
levels (LA, ω6) in response to Intralipid infusion. Without getting
into details and to keep it as simple as possible, patients with higher
LA levels post Intralipid infusion were found to have
lower ω6/ω3 ratio
at baseline (before Intralipid infusion and embryo transfer) and were significantly more
successful as seen in the Figure 3 below (43.75% will have a successful pregnancy
versus 0% for patient with high ω6/ω3 ratio and therefore
less miscarriage 31.25% versus 66.7% for the high ω6/ω3 ratio group).
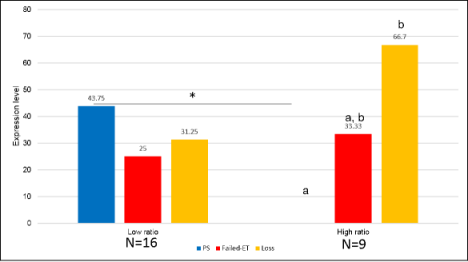
Figure 3: Transfer outcome per patient based on their ω6/ω3 at baseline.
p value <.05: *, p value <.01: **, p value <.001: ***. Different
letters mean that the difference is statistically significant, p<.05
Inversely, if a patient has high ω6/ω3 at baseline, the Intralipid
infusion will further increase her ratio, leading to an activation of
the ω6 pathway (as seen by lower LA levels post Intralipid infusion
as they are used as substrate to fuel the ω6 metabolic pathway)
leading to more inflammation.
- Lower ω6/ω3 ratio correlates with lower Th17 levels at baseline
In our data, patients with a low ω6/ω3 at baseline have also
low Th17 levels that have been linked to pregnancy losses in our data set.
So having lower ω6/ω3 ratio could be of benefit for the outcome
of a pregnancy.
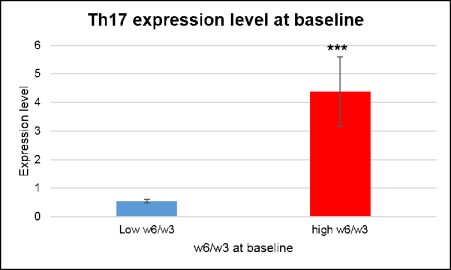
Figure 4: Th17 levels at baseline in relation to basal ω6/ω3 ratio.
p value <.05: *, p value <.01: **, p value <.001: ***.
- Omega 3 supplement: the best option to restore optimal parameters
These findings led us to hypothesize that
ω6/ω3 ratio at baseline is
a key factor determining the potential for a pregnancy to succeed.
As explained in this blog, ω6/ω3 directly reflects your fatty
acid content and your potential to preferentially activate the ω6
(pro-inflammatory) or ω3 metabolic pathway (anti-inflammatory).
At Braverman Reproductive Immunology, we are now systematically screening all our patients for fatty acid levels
and using them to determine three parameters:
- ω6/ω3 ratio
-
Potential for inflammation reflecting the direct competition between EPA and arachidonic acid in
triggering pro- versus anti-inflammatory pathway. It has been shown to
be more elevated in patients with inflammatory conditions (24).
-
Omega 3 Index: this index reflecting the long-term intake of EPA+DHA has been largely
used in the cardiovascular medical field to determine patients who are
in a protective zone versus those at risk for cardiac arrest.
During pregnancy, higher omega 3 index have been linked to reduced risks
for preterm birth (25).
Based on these parameters, patients are categorized into one of three categories:
- Low risk
- Intermediate risk
- High risk
Specific dose of EPA+DHA are recommended to restore optimum parameters
before embryo transfer or attempt to conceive. A maintenance dose is then
recommended to maintain the patient in the low risk category throughout
the pregnancy.
References