In our previous blog, we introduced you to a novel category of miscarriages
grouped under the term,
Correctible Reoccurring Aneuploid Conversion Syndrome (CRACS).
By treating endometriosis, PCOS or obesity among other causes potentially
leading to CRACS, we have been able to significantly improve outcomes
in those patients that conceived under our care.
- Who are the CRACS patients?
CRACS patients are women who have no significant issues conceiving, but
who experienced recuurent implantation failure and/or recurrent pregnancy
losses (RPL) with at least one of the miscarriages characterized as aneuploid
(embryo genetically abnormal), that can be documented by:
- Chromosomal genetic testing on the product of conception (POC).
- A chemical pregnancy (a very early loss taking place before any confirmation
by an ultrasound scan) that is more likely to be considered as aneuploid (1).
- A loss occurring before 8 weeks with no prior fetal heart beat (FHB) detection.
In Recurrent pregnancy losses (RPL), most of the miscarriages have been
attributed to aneuploidy (abnormal karyotype) and can account for up to
80% of all losses in the general population (2) although the more losses
you have, it is thought that it is less likely losses are aneuploid (for
more information, read our blog).
Besides oocyte aging, which is one of the main factors involved in aneuploid
embryonic losses (abnormal genetically), conditions such as Endometriosis
and/or PCOS significantly impact the egg reserve at two levels,
egg abundance but also
egg quality.
- Pregnancy success at Braverman Reproductive immunology in CRACS patients
Patients who had immune testing performed with us and who did experience
at least 2 losses with a minimum of one documented aneuploid loss, prior
to our care, were included in the study.
Based on their immune results, physical examination, Doppler and ultrasound
scans prior to conception (natural conception or IVF cycle), patients
received our tailored therapy including but not limited to immune therapy,
endometriosis resection by our robotic laparoscopy specialist, treatment
of PCOS by metformin, mitochondrial function supplements , the treatment
being maintained at least through the first trimester.
Results of our retrospective study, including N=155 patients, showed that
78.7% had a successful pregnancy as defined by a live birth or an ongoing pregnancy
past 12 weeks (p=.0001, a low p value means that the results are highly
significant).
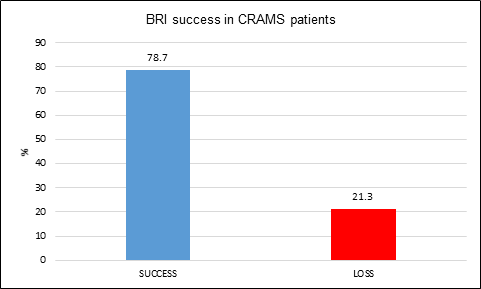
Figure 1: Pregnancy success at Braverman Reproductive Immunology in the CRACS population
and after adequate therapies (this is not a guarantee of future performance).
The majority of our population (71%) had a
no prior successful pregnancies (primary infertility) and no significant difference was determined between
the types of infertility as shown in Figure 2.
- Primary has no history of a successful birth prior to the miscarriages.
- Secondary has a history of a full term birth followed by miscarriages.
- Tertiary has a history of miscarriages prior to and after a full term birth.
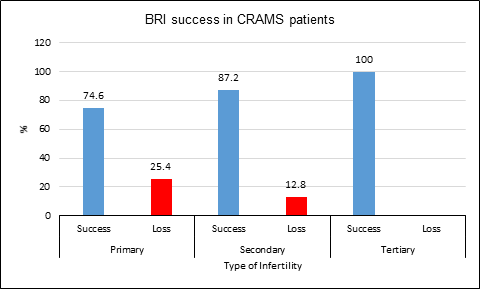
Figure 2: Pregnancy success at Braverman Reproductive Immunology in the CRACS population
and after adequate therapies based on patients infertility type.
At first attempt under our care,
70.6% of patients
will had a successful pregnancy as seen in Figure 3 (p=.0001, a very low p value shows a very high statistical
significance).
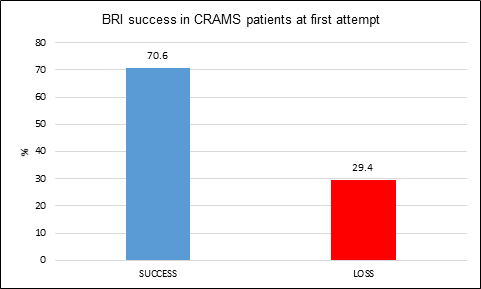
Figure 3: Pregnancy success at Braverman Reproductive Immunology in the CRACS population
and after adequate therapies at first attempt.
Our patient population is fairly young with 52% being 37 years old or
younger. Our success rate are steady among the younger patients (40 years
old or less), reaching up to
83.8% of pregnancy success (p=.0001, a very low p value shows a very high statistical significance).
Older patients (41 years and older) have a lower chance of having a successful
pregnancy, up to 69.2% (p=.04) as seen In Figure 4.
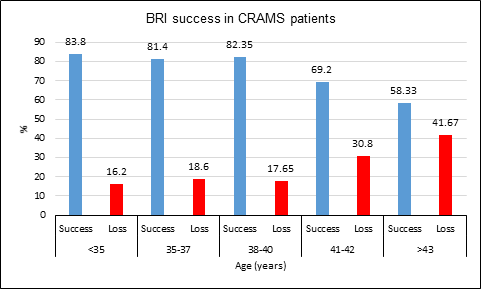
Figure 4: Pregnancy success at Braverman Reproductive Immunology in the CRACS population
and after adequate therapies based on patients age.
65% of CRACS patients are affected by Endometriosis and/or PCOS, two conditions previously shown to negatively impact oocyte/embryo quality
thus leading to miscarriages.
81.8% of our endometriosis/PCOS treated patients had successful pregnancies as
seen in Figure 5 (p=.0001).
The patients in the “other underlying issue category” had
immune related issues and were treated with aggressive immune therapies.
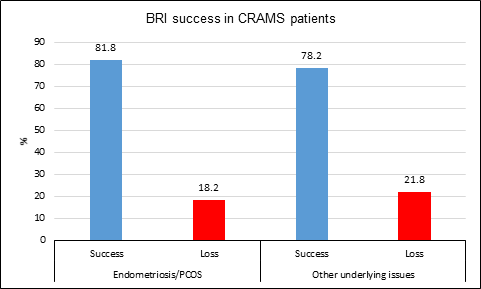
Figure 5: Pregnancy success at Braverman Reproductive Immunology in the CRACS population
based on patients underlying conditions and after adjusted treatment.
At Braverman Reproductive Immunology, we are working, on a daily basis, on optimizing our current immune screening
panel to determine parameters whose dysregulation could be involved in
your fertility issues.
We keep developing new tests and areas of research to better determine
the causes of your multiple losses and be able to treat them therefore
helping you achieve the goal of becoming a mother.
References
- Edwards RG. Causes of early embryonic loss in human pregnancy. Hum Reprod
1986; 1:185e98.
- Hodes-Wertz B, Grifo J, Ghadir S, Kaplan B, Laskin CA, Glassner M, Munné
S. Idiopathic recurrent miscarriage is caused mostly by aneuploid embryos.
Fertil Steril. 2012 Sep; 98(3):675-80.